

A Case Report from MuthuMeenakshi Hospital, Pudukkottai
Trauma in newborns and young infants is extremely rare but can be life-threatening when it occurs. Immediate recognition, rapid resuscitation, and coordinated teamwork are crucial to saving lives.
This case from Muthu Meenakshi Hospital, Pudukkottai highlights how timely neonatal trauma resuscitation, emergency blood transfusion, and neurosurgical intervention helped save the life of a 40-day-old infant.
Introduction
Head injuries in infants are particularly dangerous because of their fragile skull structure, small blood volume, and high risk of complications such as hemorrhagic shock, hypothermia, acidosis, and coagulopathy.
The “golden hour” in trauma care plays a critical role in survival. Early resuscitation and rapid surgical intervention can significantly improve outcomes.
This case demonstrates how prompt emergency response and multidisciplinary teamwork helped a critically injured newborn recover fully without neurological deficits.
Case Presentation
Patient Details
A 40-day-old female infant, one of twins, was brought to the Emergency Department with an alleged history of plastered wall tiles falling onto her head at home approximately 20 minutes prior to arrival.
There was no history of:
Loss of consciousness
Vomiting
ENT bleeding
Seizures
However, the infant had active bleeding from a large frontal scalp laceration, with the underlying skull bone exposed.
Condition on Arrival to Emergency Department
On arrival, the infant appeared critically ill.
Clinical Findings
Continuous crying
Pale appearance
Cold peripheries
Feeble pulses
Dry mucosa
These signs indicated hemorrhagic shock due to acute blood loss.
Initial Vitals
Heart Rate: 190/min
Respiratory Rate: 50/min
SpO₂: 99% on room air
Emergency Management and Resuscitation
The trauma resuscitation team was activated immediately.
Immediate Interventions
Two intravenous lines secured
Blood samples sent for emergency investigations
Direct wound compression applied to control bleeding
IV fluid bolus administered
Fluid Resuscitation:
Baby weight: 3 kg
IV fluids given: 20 ml/kg (60 ml)
Reassessment After Initial Resuscitation
Following initial management:
Vitals
HR: 160/min
RR: 50/min
The infant continued to have:
Weak cry
Ongoing wound soakage
The paediatrician arrived immediately, and emergency blood transfusion with supportive medications was initiated.
Medications Administered
The infant received:
IV Paracetamol
IV Antiepileptics
IV Antibiotics (Meningitis dose)
Laboratory Findings
Hemoglobin: 8 g/dL
Previous Hb (1 week earlier): 17.8 g/dL
This indicated significant acute blood loss.
Blood Transfusion
1 unit of packed red blood cells (PRBC) transfused in the Emergency Department.
Advanced Trauma Evaluation
The neurosurgeon, intensivist, and anesthetist were immediately alerted.
The infant was transferred for CT brain imaging, accompanied by paramedics and the critical care team.
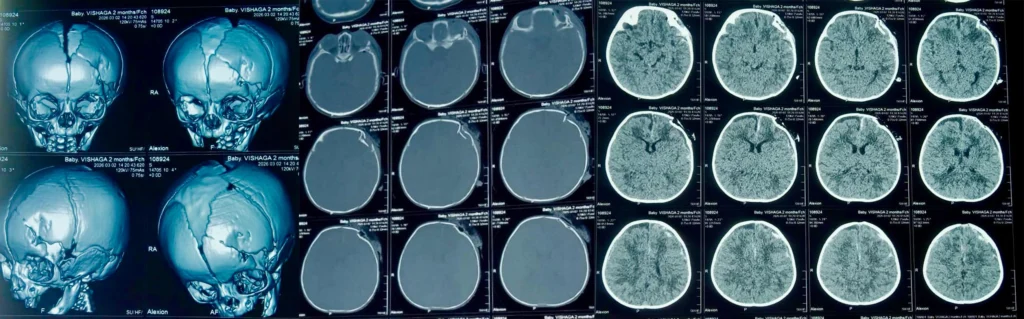
CT Brain Findings
Imaging revealed multiple serious injuries:
Depressed frontal skull fracture with bone fragments impinging on the frontal lobe
Subdural hemorrhage
Subarachnoid hemorrhage with perilesional edema
Parietal bone fracture
Hemotympanum
Pneumocephalus
Fracture extending to the superior orbital wall with air pockets
These findings confirmed severe head trauma requiring emergency neurosurgical intervention.
Surgical Management
The infant was immediately shifted from the CT suite to the operating theatre.
The surgical team included:
Paediatrician
Neurosurgeon
Intensivist
Anaesthetist
Critical care nurses and paramedics
Intraoperative Procedures
Extensive wound exploration
Thorough irrigation and debridement
Elevation of the depressed frontal bone
Hemostasis achieved
Following surgery, the infant recovered well from anesthesia and was extubated on the operating table.
She was then shifted to the Neonatal Intensive Care Unit (NICU) for close monitoring.
Post-Operative Recovery
Within 24 hours in the NICU, the infant showed remarkable improvement.
Clinical Status
HR: 130/min
RR: 40/min
Alert and active
Moving all limbs
Afebrile
Accepting mother’s feeds well
Adequate urine output
Hemoglobin
Post-operative Day 1 Hb: 10.8 g/dL
The infant was later shifted to the ward, continued treatment for five days, and was discharged on Day 7.
Outcome
The infant made a complete clinical recovery.
There were:
No neurological deficits
No residual morbidity
Normal feeding and activity
This case demonstrates the life-saving impact of rapid emergency care and coordinated multidisciplinary management.
Key Learning Points from the Case
Golden hour management significantly improves neonatal survival and reduces hospital stay.
Team-based trauma response is critical for successful neonatal resuscitation.
Neonatal trauma differs from adult trauma, with increased risk of hypothermia, acidosis, and coagulopathy.
Early blood transfusion can be lifesaving in acute pediatric hemorrhage.
Controlled and targeted resuscitation is more effective than aggressive fluid overload.
Acknowledgement of the Trauma Care Team
This successful outcome was made possible by the dedicated teamwork of multiple specialists.
Heartfelt thanks to:
Dr. Periyasamy – Managing Director
Dr. Andrew Stephen – Paediatrician
Dr. Ramesh Raja – Neurosurgeon
Dr. Archana – Intensivist
Dr. Narayanasamy – Anaesthetist
Dr. Ramsundar – Consultant, ICU Team
Emergency Department Doctors
Emergency Paramedics and Critical Care Nurses
Hospital Administration and Paraclinical Team
Their timely intervention, coordination, and commitment played a vital role in saving the infant’s life.
Conclusion
Severe head injury in neonates is rare but can rapidly become fatal without early recognition, rapid trauma resuscitation, and neurosurgical care.
This case highlights the importance of:
Emergency trauma preparedness
Multidisciplinary collaboration
Timely surgical intervention
At Muthu Meenakshi Hospital, Pudukkottai, advanced emergency care and coordinated teamwork helped give a 40-day-old infant a second chance at life.


